(515) 280-3100
(515) 280-3100
An Anatomic Obstruction
Written by: Meghann R. • 2017 Scholar
 Signalment & Presenting Complaint
Signalment & Presenting Complaint
Charlie: 4 year old neutered male mix breed canine
Presenting complaint:Non-specific GI sympotoms, restless, reluctant to jump up
Major Rule outs:
- Foreign body obstruction
- Gastric Dilatation & Volvulus (twisting of the stomach)
- Pancreatitis
- Infectious disease (parasites, bacteria)
- Neoplasia (lymphoma, adenocarcinoma)
Physical Exam
During the physical exam Dr. Thomsen noted a possible mass in the amdomen that caused discomfort. No other abnormalities were noted.
Next Step: Bloodwood and Abdominal X-Rays.
Charlie’s Test Results
Bloodwork
CBC
- Hemoconcentration (high packed red blood cell volume likely due to dehydration)
- Mature neutrophilia and lymphopenia– high neutrophils and low lymphocytes
- consistent with a “stress leukogram”
Chemistry Panel
- Mild hypokalemia (low potassium)- potentially due to loss of potassium through the gastrointestinal tract
Interpretation: IV fluids are recommended to correct the dehydration. The other abnormalities are not linked to any definitive diagnosis and therefore did not need to be immediately corrected prior to treatment.
 X-Ray
X-Ray
- Yellow Arrow: Circular dilation of the intestine in the caudal abdomen was found cranial to the urinary bladder. Repeat X-rays did not show any movement of the material through the intestinal tract.
- Gas is found throughout the intestinal tract (Red Arrow)
- Other abdominal organs (liver, kidneys, spleen, urinarybladder were normal size and lacked mineralization
- No skeletal abnormalities such as spinal fusion, fractures, or dislocations were noted
Interpretation: No signs of GDV or abdominal masses that are consistent with neoplasia were identified. This X-Ray shows a likely foreign body obstruction
Diagnosis
Charlie was diagnosed with an intestinal foreign body located approximately in the colon (last section of intestine before the rectum).
Next Step: Abdominal Exploratory Surgery (surgical incision into the abdomen to locate the foreign body)
Surgery
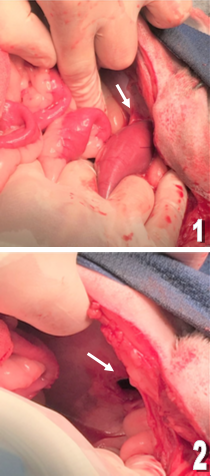 After incising the abdomen, initial exam of the intestine did not reveal ant obvious signs of an obstruction
After incising the abdomen, initial exam of the intestine did not reveal ant obvious signs of an obstruction- Further exam did reveal an adhesion of the intestine to the left body wall at the same location as the foreign material identified on X-Rays (Image 1)
- The adhesion was manually broken down where a 1.5 cm diameter body wall defect was identified (Image 2)
- The body wall defect was closed using suture material
- The previously adhered section of intestine contained sponge-like material with consistency similar to the foreign body material identified on X-Rays
- Resection & anastomosis of the affected intestine (damaged intestine was removed then new viable ends were reattached)
- The surgical site was closed and skin staples were applied. The patient recovered smoothly post-op and was sent home the following day
- Medications:
- Tramadol (pain)
- Carprofen (anti-inflammatory)
- Famotidine (antacid)
- Cerenia (anti-nausea)
Wait ... What about antibiotics?
- For many soft tissue surgeries antibiotics are actually contraindicated.
- Oral antibiotics post-op can actually mask symptoms of septicemia and prevent timely medical intervention.
- By the time septicemia is detected, often times it is too late to save the patient.
- If antibiotics are used it is recommended that they only be administered perioperatively or immediately post-op via
- IV. This patient was given Cefazolin (the recommended drug) IV immediately following surgery.
Prognosis
Overall excellent prognosis. The majority of the intestine was viable at the time of surgery, intestine was checked for any leakages prior to closure and none were observed.
Things to monitor that can greatly affect outcome: septicemia from leakage of intestinal contents at the surgical site, continued vomiting/diarrhea, surgical site dehiscence (incision site on abdominal wall opening up), necrosis of intestine from incomplete resection