
DKA Case Report
Written by Ashley Burrows • 2019 Scholar
History

Gir is a thirteen year old neutered male that presented to his primary care veterinarian because he was vomiting food and water, lethargic, anorexic, and had lost four pounds in a month (weighing in at 20.1 pounds). His original blood glucose was very high at 555 mg/d. Gir’s doctor diagnosed him with diabetic ketoacidosis and referred him to Iowa Veterinary Specialties.
Physical Exam Findings
Gir’s physical exam revealed a left sunken eye that was consistent with an ulcer in the medial aspect of the eye. He had tacky mucus membranes indicating dehydration, was lethargic, had a slightly distended abdomen, slightly increased respiratory rate, and a depressed nervous system. Cardiac disease was also a concern due to the presence of a systolic murmur (3/6).
Diagnostic Results
Based on Dr. Chrouser’s and the regular DVM’s findings, further diagnostics and treatment began immediately. Gir’s blood tests revealed an elevated glucose (629), blood urea nitrogen (BUN 76), alanine aminotransferase (ALT 244), cholesterol (422), gamma-glutamyl transferase (GGT 29), alkaline phosphatase (ALKP greater than 2000) and lipase (4103). Other information faxed from the rDVM included a complete blood cell count (CBC) which showed mild leukocytosis with neutrophilia and an abnormal canine pancreatic lipase test. Urine analysis showed specific gravity of 1.024, with bacteria, ketones, protein, and glucose present in the urine sample. Radiographs showed hepatosplenomegaly (enlargement of the liver and spleen).
Gir’s high blood glucose level is explained by the fact that his body is struggling to produce enough insulin to drive glucose into cells. Instead of glucose being in cells, an unusually large amount is floating around in the blood stream. The body’s cell membranes are mostly impermeable to glucose, explaining why glucose cannot diffuse into cells without insulin. Instead, the highly concentrated glucose causes an osmotic gradient (fluids flow from low concentration to high concentration) and fluid is drawn from the intracellular space into the vascular and interstitial spaces. Glucose remaining in the blood is filtered at the glomeruli in the kidney and excreted through the renal tubules. The kidneys struggle to retain the glucose, leading to its excretion and presence in the urine. Water follows this sugar leading to dehydration even when the animal is compensating by drinking more water. (Thomovsky)
The serum biochemistry test commonly also reveals high cholesterol and persistent to mild elevated liver enzymes (like alkaline phosphatase and alanine aminotransferase) because of the fatty changes and buildup in the liver. This happens because the body is not able to adequately use glucose for energy and needs to use other sources leading to an increased activity of hormone-sensitive lipase in adipose tissue and mobilization of fat stores which gets sent to the liver. GGT is also elevated because of the oxidative stress put on the liver. The abnormal canine pancreatic lipase reflects the inflammation of the pancreas. (Davison)
The complete blood cell count revealed leukocytosis (high white blood cell count) and neutrophilia because of the inflammation and oxidative stress caused by the presence of ketones in the body. Neutrophils typically rise in the body when it is responding to an acute illnesses and the body’s inflammation processes. The white blood cells levels will rise as their production increases and they are released quicker, due to the increase in proton ions in the blood stream. These two states are commonly found in tandem with DKA. (Xu et. all)
A urine sample was recommended because the increase of glucose in the urine increases the risk of bacterial urinary tract infection (UTI), which can lead to an increase in insulin resistance and lead to even more challenges in stabilizing the diabetic patient. The urine analysis also allows a chance to test the urine for the presence of ketones. (Davison)
Diagnosis
Gir was in critical condition when he arrived at IVS and needed to be immediately treated for diabetic ketoacidosis. A diabetic dog is unable to move glucose from the bloodstream into cells to fuel cellular metabolic process. This causes the cells of the body to find alternative energy sources like fats and proteins to provide fuel for the metabolic processes. At first, the body is able to supply enough energy to the cells, but while breaking down the fats to make energy, ketoacids are formed in excess. Oxidation of fats to form ketone bodies frees carboxylic acids that releases hydrogen ions. Therefore, an overproduction of ketone bodies leads to an overproduction of hydrogen ions, leading to a decrease in pH and acidosis. (Thomovsky)
There is also a reduction in adipose fatty acids and increase in lipolysis, leading to an increase in circulating lipids (fat) which end up aggregating in the liver. Gir had hepatomegaly (enlarged liver) because he could not deal with the amount of lipids in his liver. (Niaz et al. 2018)
Treatment
Dr. Chrouser recommended hospitalization with him on an insulin fluid tree, monitoring of blood glucose, IV fluids and supportive care. This treatment is in line with literature suggestion of immediate fluids and insulin therapy (Thomovsky). Gir had a jugular catheter placed, instead of a cephalic catheter like most of our hospitalized patients. This made it easier and less painful for him when we needed to draw blood every couple hours to test his blood glucose levels.
Medications
Diabetic patients will be reliant on insulin for the rest of their lives. Gir’s pancreas (islets of Langerhans) struggles to produce insulin. Giving insulin injections will resolve the patient’s hyperglycemic state by storing circulating glucose in the liver as glycogen. Insulin also transports glucose into cells to be used in glycolysis and the tricarboxylic acid (TCA) cycle. The goal of insulin treatment is to maintain the patient glucose concentration anywhere from 100 to 250 mg/dL. (Thomobsky)
An insulin tree is used to return the animal to a normal energy state. This requires the animal to discard the ketones built up in their body. The insulin tree is done during hospitalization. A blood glucose test is ran every 2 hours to monitor the glucose levels. This was done by drawing blood from the jugular catheter and using a glucometer. Based on the glucose reading Gir’s fluids were adjusted. If the glucose level was high, more insulin was added to his IV catheter, and if the glucose was low, more dextrose (sugar) was added. Dextrose supplementation does the opposite of glucose and draws the glucose out of cells when the patient’s serum glucose concentration dropped too low. Gir was taken off the insulin tree when there were no longer ketones present in his urine.
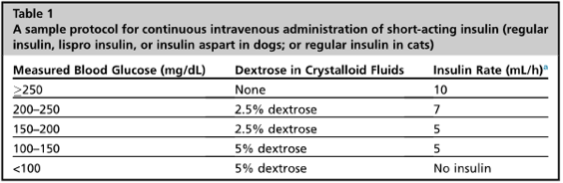
Figure 1. Example of the insulin tree protocol followed at IVS (Thomobsky).
Figure 2. AlphaTrak glucometer used in testing Gir’s glucose level. (Davison)
His intravenous fluid was Normosol-R supplemented with 7 mEq KCl (potassium chloride). Giving this crystalloid fluid is necessary to shift fluids naturally from the animal’s intravascular space back into interstitial and intracellular space (Thomovsky).
He was also placed on IV unasyn (ampicillin/sulbactam) to treat his urinary tract infection. It is an antibiotic to fight generalized bacterial infections. Maropitant was also prescribed as an antiemetic for Gir. This was to help control his vomiting and prevent further stomach issues. (Plumb).
Prognosis
Prognosis for dogs with DKA is guarded, because it requires hospitalization (2-3 days) to stabilize the patient’s glucose and can be very costly. It also requires a long term treatment plan with the patient reliant on lifelong insulin injections and a compliant owner.
Gir Today

Gir was discharged to his owner when he no longer had ketones appearing in his urine and his blood glucose was stable. His owners will be in charge of giving him insulin injections twice a day for the rest of his life, and he was recommended to go to his regular DVM in two weeks for a blood glucose check.
Gir’s diet will also be vital in ensuring his glucose levels are stable. He needs to eat the same amount of food, same type, and at the same time every day to maintain and control his glucose. Ideally Gir would be fed twice a day within one hour of insulin injection. (Davison) It is recommended to feed Gir a fat-restricted diet that is high in fiber and complex carbohydrates. (Silverstein and Hopper) Dr. Rupiper at IVS recommended a low fat diet like Hills weight and digestive management at Gir’s discharge.
References & Citations
- Davidson, Lucy. (2018). Diabetes Mellitus in Dogs. In Practice. https://inpractice .bmj.com/.
- Plumb, Donald. (2018). Plumb’s Veterinary Drug Handbook. Hoboken, NJ: Wiley-Blackwell.
- Niaz, Kamal, Faheem Maqbool, Fazlullah Khan, Fatima Ismail Hassan, Saeideh Momtaz, and
Mohammad Abdollahi. (2018). Comparative Occurrence of Diabetes in Canine, Feline, and Few Wild Animals and their Association with Pancreatic Diseases and Ketoacidosis with Therapeutic Approach. Veterinary World. - Silverstein, Deborah and Kate Hopper. (2015). Small Animal Critical Care Medicine. St. Louis, Missouri: Elsevier.
- Thomovsky, Elizabeth. (2016). Fluid and Electrolyte Therapy in Diabetic Ketoacidosis. Veterinary Clinic Small Animal, Elsevier Inc. https://dx.doi.org/10.1016/j.cvsm.2016.09.012.
- Xu, Wei, Hai-feng Wu, Shao-gang Ma, Feng Bai, Wen Hu, Yue Jin, and Hong Liu. (2013). Correlation between Peripheral White Blood Cell Counts and Hyperglycemic Emergencies. International Journal of Medical Sciences, 10 (6), 758-756. doi:10.7150/ijms.6155