
Feline Infectious Peritonitis
Written by Kaylee Endres • 2017 Scholar
History and Physical Exam
Owner brought a 9.5 year old altered male domestic short hair into Iowa Veterinary Specialties that presented as lethargic with a decreased appetite for the past week. The patient was reluctant to move while at home and was not responding to his name being called by owner. No current or prior diarrhea or vomiting and patient had not eaten in the past 12 hours. Patient is strictly an indoor only cat with other feline housemates.
Upon physical exam -
- Mucous Members were light pink
- No pain upon abdominal palpation
- Tachypnea (increased breathing rate at 50 breaths per minute: normal range for a cat is 16-40)
- Increased efforts to breath with clear lung sounds
Patient was placed into an oxygen cage to help stabilize his breathing.
Diagnostic Procedures
Thoracic and abdominal radiographs
Blood work: complete blood count (CBC) and a Comprehensive Chemistry
Feline Triple SNAP Test: blood test that screens cats for feline immunodeficiency virus (FIV), feline leukemia virus (FeLV), and feline heartworm antigen (FHW)
Thoracocentesis (surgical puncture of the chest wall by a needle to extract fluid or air from around the lungs)
Diagnostic Findings
CBC
- RBC - Red blood cell count 6.26
- PCV - Packed cell volume 35%
- TP - Total protein 10
- Neutrophilia - Elevated neutrophils 11,783
- Lymphocytosis - Decreased lymphocytes 9,268
- Non-regenerative anemia
Chemistry
- BUN – Blood Urea Nitrogen 12
- Ca – Calcium 7.7
- Glob – globulins 8.0
- Alb/Glob – albumin/globulin ratio 0.3
- K – Potassium 6.9
- Cl – Chloride 110
Feline Triple SNAP
- Negative
Radiographs
The diagnostic report from the thoracic radiographs stated severe pleural effusion in pleural cavity, which means in the space between the chest wall and the heart and lungs there was a large amount of free fluid present. In the abdomen there was poor serosal detail with small amounts of stool in the colon.
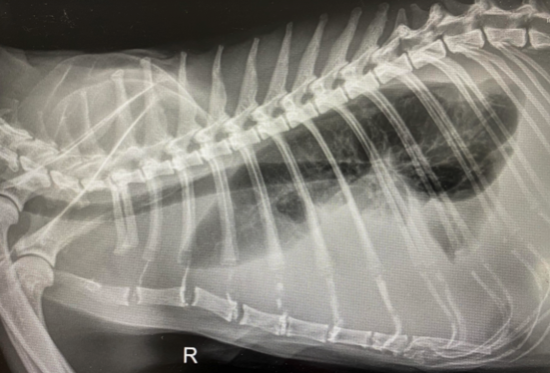
The pleural effusion is indicative of the radiopaque (uniformly white color) surrounding the lungs that show up as radiolucent (dark).
Thoracocentesis
Straw color fluid.
FIP - Prognosis Grave
Currently, there is no single test to confirm diagnoses of Feline infectious peritonitis; is extremely difficult disease to diagnose. The background patient history and clinical presentation are important factors to consider when ruling out FIP. Most commonly FIP occurs in male cats from the age of 3 and under but is also seen in older ages due to experiencing recent stress, such as homelife changes, vaccination, recent adoption of itself or another pet, and so on. The clinical signs to be aware of are fever of an unknown origin, anorexia, weight loss, effusions, icterus, or neurological symptoms. The vagueness of the clinical signs shows why FIP can be problematic to diagnose and why it should always be on the differential list until further diagnostic tests can be ran.
The laboratory tests and analysis of effusion samples help to determine the definitive diagnosis of FIP. Common blood work findings are lymphopenia, neutrophilia, low albumin to globulin ration. In FIP patients, when the albumin to globulin ratio is lower than 0.4 it is very suggestive of FIP. The clinician would want to see a score of 0.6 or above to be able to rule out FIP as a differential. Patients with FIP will have an effusion sample that appear straw yellow in color, viscous, protein rich, with low cellularity. If there is still concern for further diagnostics tests to help support or rule out FIP there are additional specialized tests that can be performed. Unfortunately, in this case that was brought to IVS further diagnostics were not needed due to the patient’s current declining state, safety of the remaining household cats, and the discussion of a humane euthanasia.
The prognosis for FIP-positive cats is often grave. The mortality is close to 100% of confirmed cases. There are two different types of FIP (wet and dry form). The wet form or effusive form is often more fatal and faster decline than the dry form. This poor prognosis is due to the unstoppable disease progression and there being no effective treatments. Another important factor to consider when dealing with a FIP-positive case is the other cats in the same household. Since there is no current vaccine for FIP and it is transmitted via fecal oral route it is crucial to maintain appropriate hygiene of the litter pans in a multi-cat household while also keeping the food and water bowls separate from the litter pans. This will help to reduce the risk of possible transmission.
References & Citations
- Addie D, Belak S, Boucraut-Baralon C, Egberink H, Frymus T, Gruffydd-Jones T, Hartmann K, Hosie MJ, Lioret A, Luts H, Marsilio F, Pennisi MG, Radford AD, Thiry E, Tryyen U, Horzinek MC. Feline infectious peritonitis: ABCD guidelines on prevention and management. Journal of Feline Medicine and Surgery 2009; 11: 594- 604.
- Wong, Chris; DVM. Thoracocentesis. Clinician’s Brief. Respiratory Medicine. June 2007. https://www.cliniciansbrief.com/article/thoracocentesis
- SNAP Feline Triple Test. IDEXX. January 1, 2020 – December 31, 2020. https://www.idexx.com/en/veterinary/snap-tests/snap-feline-triple-test/
- Pleural Effusion. Metropolitan Veterinary Associates, Inc. 2626 Van Buren Avenue Norristown, PA 19403. Retrieved June 21, 2021. https://metro-vet.com/references/pleural-effusions/
- Radiographs of right lateral thoracic view. [Digital image]. (2021). Retrieved June 24, 2021 from IVS Emergency Hospital.